Welcome to Smoke-Free Life: Your Guide to a Healthier You!
🚭 Ready to quit: secondhand smoke and live a healthier life? Smoke-Free Life is here for you! Our easy-to-use app is like having a friend to help you through a program that checks where you are, helps you change your habits, and keeps track of your progress.
🔍 Check Yourself:
Answer some simple questions about yourself and your exposure to smoke using our easy survey.
Join our program with a quick scan of a QR code, and you’ll unlock a bunch of cool features like videos, chats, and support messages.
📱 Change Your Habits:
Get fun and interesting content, quizzes, and messages to help you stop smoking and stay healthy.
Share what you learn with your friends on Facebook, WhatsApp, and more to spread the word.
Talk to others in our app about your journey and get support and answers to your questions.
📊 See Your Progress:
We’ll check in with you after 1 month, 2 months, and 6 months to see how you’re doing.
We want to know what you think and how you’re feeling, so we can help you even better.
🌟 Why Choose Smoke-Free Life?
It’s like having a personal coach for your health journey.
Easy-to-use app with fun activities.
Connect with others for support and encouragement.
Get real-time help through chat and messages.
Keep getting better with regular check-ins.
Ready to live smoke-free? Download Smoke-Free Life now and start your journey to a healthier and happier you!
Assessment of Second-hand Tobacco smoke (SHS) exposure and evaluation of mHealth promotion strategy among attendants of cancer patients at a tertiary cancer hospital
Principal Investigator:
Dr. Jitendra Kumar Meena
Assistant Professor (Preventive Oncology)
National Cancer Institute (NCI), Jhajjar
Co- Investigator:
Dr. Hari Krishna Sagiraju
Preventive Oncology, NCI Jhajjar

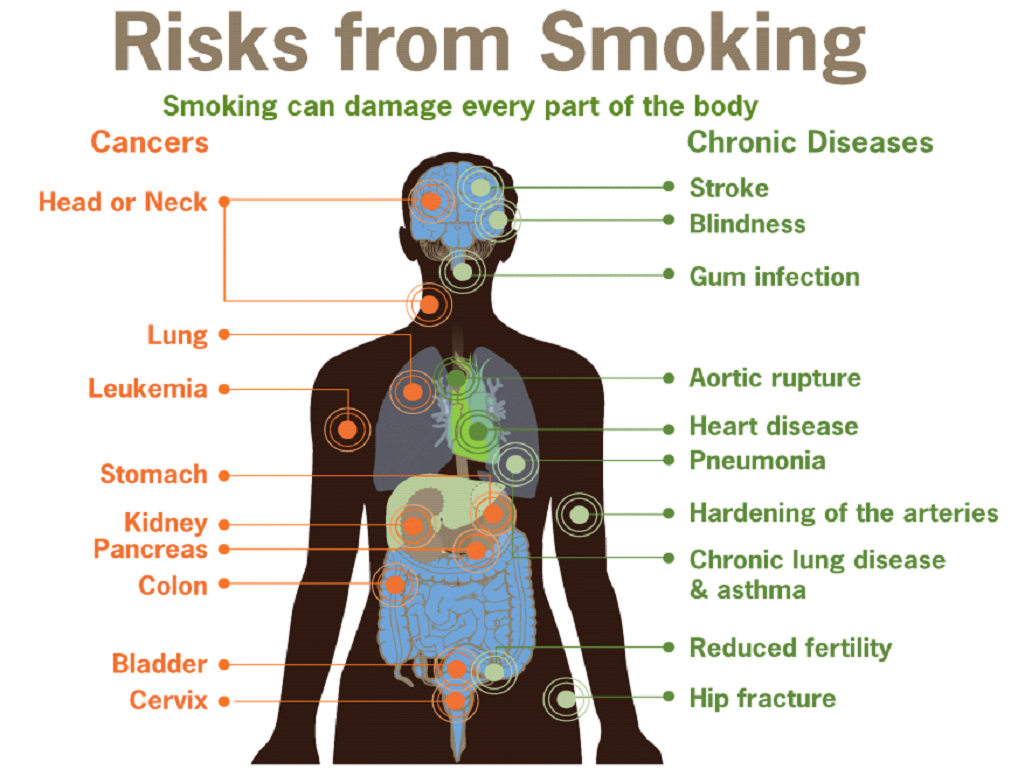
Second-hand tobacco smoke (SHS) has been classified as a “Group 1” carcinogen by the International Agency for Research on Cancer (IARC). Apart from cancers, SHS leads to ischemic heart disease, lower respiratory infections, otitis media, tuberculosis, and asthma,X etc.1,2 Despite anti-smoking regulations, as per Global Adult Tobacco Survey (GATS) – 2, high SHS exposure is recorded in Delhi’s public places (28.0%) compared to the national average (23.0%). There are deficient data and literature pertaining to the burden of SHS, its impact, and strategies for control in the Indian subcontinent. Communication research is a powerful tool in developing healthy behaviors among people. This project aims to assess SHS exposure and Knowledge, Attitude and Practices (KAP) and impact of mHealth behavior change communication (BCC) strategy for SHS prevention among attendants of cancer
patients.
A pilot mixed method, interventional study will be done for a period of 2 years. Baseline assessment of SHS will be done using an e-SHS survey. Post assessment, m Health interventions will be done for a period of 1 month. Follow-up assessment will be done at 1 month and 2 months and 6 months the qualitative evaluation will be done using in-depth interviews (IDI’s), discussions, personal feedbacks.
This study will provide an estimation of SHS burden and Improve KAP in participants to SHS. The learnings from the project will help to develop operational guide for implementing effective mHealth communication strategies. This pilot research will guide further multicentric research projects across cancer care institutions in India translating into nationwide “Stop SHS” health promotion campaign.
Project Implementation Plan:
In the initial phase of the project, baseline assessment of SHS will be done using e-SHS survey.
A. E-SHS survey: Baseline socio-demographic, SHS exposure and KAP data of study participants using an e-SHS survey which will be adopted from GATS 2 survey using standard methodology. Subsequently the study participant will be enrolled for mHealth protocol (endSHS WhatsApp broadcasts/google group/SMS and chat support) using customized QR codes.
Handheld digital devices (mobile/tablets) will be used to record responses using online survey to facilitate administration, collection, and management of survey data designed to run on an Android-based handheld portable device (tablet/smartphone).
The sociodemographic details will include age, gender, education status, occupation status, region, and residence (urban/rural). Further details on smoking exposure, compliance with smoke-free legislation, attitudes and perceptions towards various tobacco control policies and explore participants’ knowledge of the harmful effects of SHS will be obtained. Second-hand smoke exposure data of past 30 days at other public places, like government buildings/offices, private offices, health care facilities, restaurants, public transportation, bars/night clubs and
cinema hall/theatre.(4,28) Data on Smoke-free Message Sources (Media: TV; Radio; Print; Outdoor; Signage; Publications) and message recall will be obtained. For evaluating KAP of participants individual items will be scored. For eg: KnowledgeSmoking near others is harmful (Yes/No; 1/0), Smoking banned at public places, Health risks of SHS exposure, etc. For Attitude Likert scoring for items like Public places should be smokefree (Strongly agree 2, Agree 1, Neutral 0, Disagree -1, Strongly disagree -2) will be done. For Practice & Behaviors: requested others to putout STPs (Yes/No; 1/0) etc.
Post assessment phase the study participants will be delivered mHealth communication interventions.
It will involve an experimental or active strategy using mHealth services to deliver interactive content, and multimedia health messages. This will include participation in end-SHS WhatsApp broadcast groups/SMS, discussions in google groups and chat support for feedback and queries for a period of 2 weeks. Social media strategies like sharing or forwarding health messages in their social networks will be encouraged for WhatsApp, Facebook, and Twitter, etc. The BCC strategy will be developed in both English and Hindi and will be provided as per the subject preference for mass outreach. Strong evidence indicates that mass-reach health communications reduce SHS exposure, tobacco use among youth and adults, increase quit attempts, increase the use of cessation services, and prevent youth initiation when part of a comprehensive tobacco control program. (29-31)
Health communication will focus on:
1. Motivating tobacco users to quit.
2. Sensitizing active & passive smokers to the harms related to SHS.
3. Protecting people from the harms of second-hand smoke exposure
4. Improving the KAP of participants pertaining to SHS exposure.
5. Reduce the social acceptance of SHS. etc
Participant Interviews, Discussions & Feedbacks (Qualitative):
During the intervention and evaluation phase study participants will be asked to discuss and provide regular feedback on delivered material. Selective online IDIs and group discussions will be conducted and moderated by project officer. A minimum of 8 participants will be required for conducting group discussions. Due considerations of privacy and anonymity of participants will be done for reducing misreporting of information.
The effectiveness of health messages will be evaluated on the basis of ability to:
• State the issue (e.g., second-hand smoke exposure is dangerous to non-smokers)
• Include credible supporting facts (e.g., second-hand smoke contains nearly 70 chemicals that
cause cancer)
• Evoke a shared value (e.g., everyone has the right to breathe clean air)
• Include a call to action (e.g., protect loved ones from second-hand smoke).(32)
Feedbacks on overall strategy in enabling participants in the listing of obstacles to taking the action for positive health behaviour, the benefits of taking the action, The channels and activities of interpersonal communications and outreach, recall and sharing of campaign message(s), The look and tone of materials will also be taken. BCC (interactive multimedia messages, tasks etc) content will be developed and designed by project investigators with consultations with subject experts. The developed material will be checked, and pilot tested for content, accuracy and readability. A standard policy will be drafted for developing and approving health messages, maintaining privacy, responding to public comments, what can and cannot be shared on social media groups, The language and tone of social media communications and protecting the privacy of staff and clients when using photos or quotes.
Post intervention, follow-up e-SHS survey will be done at 1 month, 2 months and 6 months respectively. Follow-up data will be analyzed for evaluating the impact of intervention based on e-SHS, and KAP survey scores. The existing departmental resources will be used to interview (IDI’s) participants and will be requested to provide feedback and personal experiences as text or audio-visual messages. The COREQ (COnsolidated criteria for REporting Qualitative research) Checklist will be used for reporting qualitative findings. (33) Positive health behaviors (Qualitative) change pertaining to SHS will be assessed based on:
1. Internal Factors: Knowledge, Risk perception, Myths & misconceptions, Care seeking practices, Stigma, Self-efficacy, Self-perception, and outreach.
2. External Factors: Socio-economic characteristics, Cultural factors, access to information, Social messaging, and outlook.

